- Collection:
- Georgia Government Publications
- Serial:
- Physician profile.
- Title:
- Physician profile: toward the year 2000
- Creator:
- Georgia. Joint Board of Family Practice
- Contributor to Resource:
- Georgia. Joint Board of Family Practice.
- Publisher:
- Atlanta, Ga. : Georgia. Joint Board of Family Practice
- Date of Original:
- 1990
- Subject:
- Physicians--Georgia--Periodicals
Medicine--Specialties and specialists--Georgia--Periodicals
Medicine--Specialties and specialists
Physicians - Location:
- United States, Georgia, 32.75042, -83.50018
- Medium:
- state government records
- Type:
- Text
- Format:
- application/pdf
- Description:
- Title from cover
- External Identifiers:
- Call Number GA C910 .S1 P5 1990
- Metadata URL:
- https://dlg.galileo.usg.edu/id:dlg_ggpd_y-ga-bc910-b-ps1-bp5-b1990
- Digital Object URL:
- https://dlg.galileo.usg.edu/do:dlg_ggpd_y-ga-bc910-b-ps1-bp5-b1990
- Language:
- eng
- Holding Institution:
- University of Georgia. Map and Government Information Library
- Rights:
-

Toward the Year 2000
__
1
PREPARED BY THE JOINT BOARD OF FAMILY PRACTICE - STATE OF GEORGIA
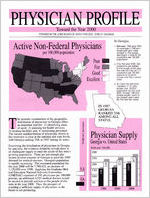
I Active Non-Federal Physicians I per 100,000population J
In Georgia:
W e e n 1986and 1990, an average of 340 physicians per year were added to the supply, resulting in a rate of 156 physicians per 100,000 population.
rIf by the year 2000,340
ph sicians are added to he supply each year,
7 the rate will on1 be 177
physicians per 00.000 persons (a 13.5% increase over the current rate). To meet the GMENAC standard of 191 physicians per 100,000 po ulation by the year 2& ,at least 450 physicians would need to be added each year for the next ten years.
n he periodic examination of the geographic distribution of physicians in Georgia offers an important tool for: 1) identifying areas of need; 2) planning for health services; 3) locating facilities and; 4) monitoring personnel. The current maldistribution of physicians shown in this overview is clear at the national and state levels, with Georgia ranking 35th in 1987 among all states.
Examining the distribution of physicians in Georgia by specialty, the evidence distinctly reveals there is an inadequate supply to meet the needs of this state's growing population. There are not enough physicians in most counties of Georgia to meet the 1990 demand for medical services. Georgia's population is rapidly increasing. The estimated population for the year 2000 will be 7,780,422, an increase of 1,150,000 over 1990. Applying the Graduate Medical Education National Advisory Committee (GMENAC) standard of 191 physicians per 100,000 persons, an additional 4,525 medical doctors would be needed to provide services to the people of this state in the year 2000. Thus, the prospect of reaching a sufficient supply of physicians in the future is not promising.
i RANKED 35th AMONG ALL STATES.
I
3 physiciansupply
I Georgia vs. United States
Family
I
' PHYSICIANS IN GEORGIA
1990 GMENAC REQUIREMENTS
GMENAC standard = 191
per 100,000persons
Below Standard
t7
Sixty-nine percent of all physicians are located in 9 metropolitan counties (population greater than 150,000) which represent 44% of the state's population. The maldistribution of physicians has continued since 1986 with the majority of decline occurring in rural areas.
One hundred-fifty counties in Georgia are below the GMENAC standard of 191 physicians per 100,000 persons.
Compared to 1986, the 1990 rate of phy-
sicians per 100,000 population declined
9 in 58 counties, remained unchan
8, and showed improvement in 9
.ed in
I 'RATE PER 100,000POPULATION
Between 1986 & 1990 in tieorgia:
The number of practicingSubspecialty physicians increased35.6%while the number of lnternists decreased 24.6%.
There was little change in the number of practicing Family Practice, OBIGYN, Pediatric and General Surgery physicians.
I SUBSPECIALTIES
There was little or no change in the Familv Practice. OBIGYN. Pediatric and ~eneraslurgery physician rate in rural areas.
There was a 33.3%decrease in the rate of Internists in urban areas and a 28% decrease in the total rate; however, at the same time the rate for lnternists did not change in the rural areas.
Urban areas of the state are above the GMENAC standard of 191 physicians per 100,000 persons; rural areas are 52% below the standard, while the total physician rate is 18% below this standard.
II INTERNALMEDICME
FAMILY PRACTICE
IIA I+1 GENERALSURGERY
1 I OB-GYN
, GENERALSURGERY
In Georgia, between 1986 & 1990 there was:
A major increase in the number of Subspecialties.
A major decrease in the number of Internists.
Little or no change in other primary care specialties (Family Practice, OBIGYN, Pediatrics and General Surgery).
An increase of 1,361 in the total number of physicians.
Only the following counties were above
the GMENAC standard in 1990:
. . Baldwin
Bibb
Clarke Fulton DeKalb Richmond
Chatham Floyd
Thomas
PHYSICIANS IN GEORGIA, 1986& 1990
NUMBER BY SPECIALTY
TOTAL NUMBER OF PHYSICIANS 1986 = 8,975
1990 = 10.336
It is suggested that the Georgia physician supply objective for the year 2000 be 191 physicians per 100,000 citizens. In order to achieve this, the following recommendations are offered:
Continuationof state support for current initiativesto educate, train and recruit physicians. Develop a measurable set of criteria to evaluate the effectiveness of the current state subsidized initiatives. Work with the Georgia Department of Industry,Trade and Tourism to include health care services as an integral part of economic development. Utilizeexisting resourcesto develop a strategic plan to be used by communitiesfor physician recruitment. Continue to provide state supplements to public and designated teaching hospitals to assist in defraying cost for providingmedical education, indigent and uncompensatedcare. Preventthe further erosion of federal "passthrough"funds for graduate medical education. Providesparsity grants and benefitsto primary care physiciansto practice in regionswhich are not economically viable. Strengthen regionalization of primary care services. Assist contiguous counties in needto coalesce resourcesto develop centralizedprimary health care services. Develop an aggressive marketing program on the need for physicians in Georgia.
1990 Supply
2000 Requirement
ACKNOWLEDGEMENTS: Appreciation to W. Scott Cathey, Michael R. Lavoie, DavidSearcy, and Tracie Whitus, Divisionof Public Health, and also Andrew Watry, State Composite Board of Medical Examinersin the preparationof this document.
SOURCES: U.S. Department of Health and Human Services, Graduate Medical Education National Advisory Committee (GMENAC) Summary Report. Washington, D.C., U.S. Government Pnnting Ofice, 1980. Joint Board of Family Practice,State Board of Medical Examiners and GeorgiaDHR, Georgia PhysicianSuwey, 1986,Atlanta, Georgia, September, 1987. Joint Board of Family Practice,Quality of Life and the Distributionof Physiciansin Geurgia: A DisturbingParadox, Atlanta, Georgia,December, 1989. U.S. Department of Health and Human Services, Health United States, 1989, HyattsviUe, Maryland, March, 1990. Georgia Office of Planning and Budget, 1990 and 2000 County Population Estimates. State Composite Board of Medical Examiners, 1990 Reliminary Physician License data. U.S. Department of Health and Human Services. Medicine, Seventh Report to the Presidentand Congresson the Status of Health Personnel in the United States, Washington, D.C., March, 1990.